The Methylxanthine We All Take! A Look on Caffeine and Its Pharmacology.
Introduction
Coffee has an insane amount of history. Where it comes from, its impact on the economy, the job opportunities it creates, its taste, its different coffee styles, its variation and so on... Every coffee taken should have something in common with each other, and that is — the presence of caffeine (unless you have decaffeinated which should remove most of the caffeine). Caffeine is known to be the most used central nervous system (CNS) stimulant in the world [1]. So, what does it do to our body and why do so many enjoy it?
This blog will go into details about caffeine and how it acts on the body itself. It will include its pharmacology and pharmacokinetics. Caffeine is a very interesting molecule and I think we take its action for granted seeing how complex it interacts with us.
This blog may be a bit hard for those who do not have a chemistry and/or a biology background, especially when it is about pharmacokinetics, but it shouldn't matter as it is still fun to read! I hope it can be interesting to you and that you can learn more about this mysterious caffeine molecule.

Caffeine - Its Pharmacokinetics
What is pharmacokinetics?
It describes the fate of the drug that moves through the body during absorption, distribution, metabolism and excretion. Before a drug can begin to exert any effect on the body it has to be absorbed into the body systems [2].
In simple terms: what the body does to the drug.
What is pharmacodynamics?
Is the study of the drug’s action on the body. There is a qualitative aspect such as how do they produce their effects and what are the targets for drug action [2]. The quantitative aspects are the magnitude of response, potency, therapeutic efficacy and tolerance [2].
In simple terms: what the drug does to the body.
Caffeine

Figure 1. Caffeine molecule with the oxygen in red, nitrogen in dark blue, carbon in grey and hydrogen in light blue.
Chemical Formula: C8H10N4O2 — there are 4 nitrogen and 2 oxygen as these will help to dissolve in water-like solution (hydrophilic molecule). The Lipinski's rule of five is also respected (it is a rule to determine if the drug will be orally active in humans). However, caffeine is also sufficiently lipophilic to pass through all biological membranes and readily crosses the blood-brain barrier [1].
Molecular weight: 194.19 g/mol, the Lipinski's rule of five is also respected.
Characteristics: Caffeine (1,3,7-trimethylxanthine) is a plant alkaloid [1]. It is considered as a small molecule and structurally resembles to a purine [1,3]. In pure form, it is an odourless and a bitter white powder or white glistening needles, hence the bitterness you get from your coffee as you may have over-extracted the coffee during the extraction process.
Absorption: Readily absorbed after oral or parenteral administration. The peak plasma level for caffeine range from 6-10mg/L and the mean time to reach peak concentration ranged from 15 minutes to 2 hours.
Distribution: Its volume of distribution is 0.8 to 0.9 L/kg [infants], 0.6 L/kg [adults]. Interestingly, due to its volume of distribution, caffeine will only stay in the plasma confinement. Meaning that most of the drug will stay in your bloodstream only and will not target deep tissues. Hence, it is distributed freely into the water at the intracellular tissue as it is a hydrophilic molecule but is sufficient enough to be lipophilic to cross the blood-brain barrier.

Figure 2. Similar but sightly different molecules.
Metabolism: Hepatic cytochrome P450 1A2 (CYP 1A2) is involved in caffeine biotransformation. About 80% of a dose of caffeine is metabolized to paraxanthine (1,7-dimethylxanthine), 10% to theobromine (3,7-dimethylxanthine), and 4% to theophylline (1,3-dimethylxanthine). See figure 2.
Elimination: In young infants, the elimination of caffeine is much slower than that in adults due to immature hepatic and/or renal function. Its elimination’s half-life may range between 1.5 and 9.5 hours but changes greatly between individuals due to a variety of physiological and environmental characteristics that influence caffeine metabolism. These can be: pregnancy, obesity, use of oral contraceptives, smoking, altitude and others [1].
Half-life: 3 to 7 hours in adults, 65 to 130 hours in neonates.
See DrugBank [3] and PubChem [4] for more interesting details on caffeine and its many other characteristics.
Caffeine - Its Pharmacology
I drink coffee, what does it do to me?
You probably wondered why in the title I said “The Methylxanthine We All Take!”, it is because caffeine belongs to the xanthine group. As figure 2 demonstrates, it is the addition of methyl groups (CH3 — added on each nitrogen) on a xanthine molecule. Since it is part of the xanthine group, caffeine will have similar pharmacological effects to other molecules that belong to that group such as theobromine or theophylline [1]. This includes various teas and chocolates.

What it does:
Caffeine stimulates the medullary, vagal, vasomotor, and respiratory centres which will promote bradycardia, vasoconstriction, and will increase the respiratory rate [3,4]. Interestingly, caffeine is used to treat certain types of headaches and is sometimes combined with other analgesics and is used for management of fatigue, orthostatic hypotension (less blood pressure when standing up causing dizziness), and for the short term treatment of apnoea of prematurity in infants [1,3,4].
Caffeine will induce these effects in a human body but note that certain factors can vary greatly these effects:
Mild CNS stimulation and effect on wakefulness, alertness, agitation, ability to sustain intellectual activity, mood, memory, physical and cognitive performance and decreased reaction times.
Respiratory centre is stimulated.
Stimulates diuresis.
Relaxes smooth muscles in the kidneys and lung.
Vasoconstriction in the cardiovascular system.
Stimulates cardiac muscles.
Anti-inflammatory effect.
If you notice the effects caffeine causes on your body, you may wonder how can we both have smooth muscle constriction and dilation? Later on, you will read caffeine effects on cyclic adenosine monophosphate (cAMP), where it will essentially increase cAMP. An increase in cAMP will result in smooth muscle relaxation. However, at the adenosine site of action, an increase in cAMP will result in an increased release of norepinephrine (noradrenaline) which will cause vasoconstriction. Confusing isn't? So, the question is, on which smooth muscles does norepinephrine act on? We know that at least the renal and bronchioles smooth muscles relax due to diuresis being present (the need to pee a lot/excretion of water) and that a drug named theophylline (which looks like caffeine and is in the same drug class) helps patients with their asthma. The norepinephrine is stronger at the alpha 1 receptors and causes vasoconstriction in the vascular system compared to epinephrine which has a much higher affinity on beta-2 receptors.
After doing pharmacology I do have the answers for you. Beta-1 and beta-2 receptors both stimulates adenylate cyclase to increase cAMP. Why then, do beta-1 agonist causes increased contraction of the heart muscles, while beta-2 agonists cause relaxation of the smooth muscles in the lungs? The answer is that beta-1, when noradrenaline works on it, increases cAMP which increases calcium influx into the cell, which increases action potential, contractility and heart rate. At the beta-2 receptor, when noradrenaline works on it, tyrosine kinase is activated and acts on the light myosin chain kinase and inhibits it. This will eventually cause muscle relaxation.
Factors that affect caffeine absorption, distribution, metabolism and excretion:
Pregnancy, oral contraceptives (or other medication), menopausal.
Nicotine consumption.
Weight, size, age, genes and current health.
Amount taken or if the person is used to coffee [1,3-5].
What it does as a mechanism of action:

Table 1. Demonstrates the different receptors caffeine interacts.
We need to know the mechanism of action of caffeine. This will tell us what effect caffeine has once it reaches and reacts with its allocated receptor. Above is table 1 that represent where caffeine, once absorbed, will go and interact. The main important receptor that caffeine interacts with is the adenosine receptors and the phosphodiesterase enzyme. However, a lot is unsure and unknown how much it contributes on other receptors [3,4], such that it was found that “caffeine's stimulatory action on dopamine, norepinephrine, serotonin, acetylcholine, glutamate, and GABA neurons is hypothesized to result from its ability to block the action of adenosine, which typically inhibits neuronal function” [1]. I will go through the two main ones and mention the other interactions caffeine has.
Caffeine: Adenosine Receptors & Phosphodiesterase

Figure 3. Shows the structure of caffeine and adenosine.
Caffeine will inhibit the cyclic nucleotide phosphodiesterases (PDEs) and has an antagonist effect on the adenosine receptors. The reason that caffeine interacts with the adenosine receptor is that caffeine resembles the structure of adenosine and hence will cause an effect. In this case, it acts as an antagonist meaning the caffeine molecule will go onto the receptor where adenosine usually goes and will cause no effect at all as occupying the receptor will make the adenosine molecule redundant or less effective.
It was previously thought that the increase in intracellular cyclic 3′,5′-adenosine monophosphate (cyclic AMP) due to the phosphodiesterase inhibition (the enzyme that usually degrades cyclic AMP) was the main reason why we get the effect of caffeine after ingesting it as an increase in cAMP has many physiological effects [3]. There is a focus on the antagonist action at the adenosine-receptors which is found within the plasma membrane of virtually every cell to be the main reason of having the effect of caffeine on the body especially since it is part of a xanthine group [3]. Adenosine, a nucleoside that is composed of adenine and d-ribose, acts as an autocoid (acts like a local hormone or near the site of synthesis and they generally have a brief duration). Adenosine inhibits the release of neurotransmitters from presynaptic sites at the neuron level [3]. Thus the antagonism of adenosine will promote neurotransmitter release which are; norepinephrine, dopamine, acetylcholine, serotonin, glutamate, gamma-aminobutyric acid (GABA), and perhaps neuropeptides [1,6]. Hence, when caffeine is ingested, it would explain the stimulatory effect at the heart which will cause the accelerated and that pronounced pounding of the heart [3]. This is due to the adenosine A1 receptor situated at the heart.
It is important to note that the adenosine receptor A1 and A2 are both being affected by caffeine as a non-selective competitive antagonists molecule and that caffeine is not a potent antagonist [7]. Since adenosine down-regulates the CNS activity, its inhibition will cause the stimulating activity of the medullary, vagal, vasomotor, and respiratory centres in the brain [4]. Here is the reason why you feel more awake and alert — thanks to adenosine not doing its job because it is not allowed to do it, looking at you caffeine.
Here is the interesting bit on caffeine and inflammation:

By acting as an adenosine antagonist there is also psychotropic and anti-inflammatory activities [4]. The anti-inflammatory effect is due to caffeine being non-selective competitive at the phosphodiesterase (PDEs), hence causing a sort of inhibition. The inhibition of PDEs will raise the intracellular concentration of cyclic AMP (cAMP) which will activate the kinase A and thus inhibits leukotrienes synthesis. This action will reduce inflammation [4]. Also, by blocking adenosine, the pathways that produce inflammatory molecules are blocked as a study in Nature Medicine show these results. “Caffeine may counter age-related inflammation” suggests that there is a link between caffeine and its anti-inflammatory effects.
The Main Mode of Action
Adenosine receptor, a1 & a2
How it works naturally:

Figure 4. Demonstrates the adenosine receptors.
Adenosine binds on purigenic receptors and produces a physiological effect such as vascular smooth muscle relaxation [8], which in terms leads into vasodilation. In coronary vascular smooth muscle tissue, adenosine binds to A2 receptors which are coupled with G-protein and activates the G-protein system. The G-proteins coupling system is very important in human physiology and can be seen in many cells (note: G-protein is a complicated system, I will not go into too many details on how they work). A1 and A2 receptors both use G-proteins coupling system but A1 uses Gi-protein and A2 uses Gs-protein. The G-proteins are responsible for cascading actions and up-regulation or down-regulation. As Adenosine activates the Gs-protein coupling system on the A2 receptors, the Gs-protein will stimulate adenylyl cyclase (an enzyme and seen as AC in figure 4) [8]. The adenylyl cyclase will increase the concentration of cyclic AMP (cAMP) which will activate a protein called kinase. The kinase activation will stimulate the ATP-sensitive potassium channels which are at the smooth muscle cells. These smooth muscles get stimulated and become hyperpolarized [8]. All in all, many things will act and interact causing a physiological effect which results in the smooth muscle to be relaxed. An increase in cAMP also causes smooth muscle relaxation through another pathway and there is evidence that adenosine inhibits calcium entry into the cells as calcium is needed for contractions of the cell [8].
A1 receptors are found in cardiac tissue which are coupled with a Gi-protein and has a similar but different outcome compared to the A2 cascading actions. The activation of this pathway causes the potassium channels to open and hyper-polarizes the cell [8]. Activation of Gi-protein will decrease cAMP and not increase, unlike A2 receptors activation. In short, adenosine acting on A1 receptors will inhibit the release of norepinephrine which decrease the heart rate and reduces conduction velocity [8].
How caffeine intervenes:
Caffeine molecules, which resembles adenosine molecules, is a non-selective competitive antagonist. This means that to cause the same effect as before the introduction of caffeine, we would need more adenosine molecule to compete with caffeine.
Non-selective: it will either go to A1 or A2 receptors.
Competitive: it will compete with adenosine for the same spot.
Antagonist: when it is reaching that receptor there is no effect or an inhibition effect.
Thus by going on A1: there is no receptor activation, Gi-protein is not activated, the potassium channels does not hyper-polarize, adenylyl cyclase is not activated, and most importantly there is no decrease in cAMP. Hence, adenosine is not there to inhibit the release of norepinephrine and the heart rate increases giving us that heart pounding and accelerated heart rate when drinking coffee.
On A2: there is no receptor activation, Gs-protein is not activated, adenylyl cyclase enzyme is not activated, the kinase protein is not activated, no increase in cAMP. An increase in cAMP causes vasodilation, hence with caffeine, the opposite effect will occur as vasodilation is prevented. This helps with certain headaches when there is vasodilation in the brain and which causes pain as it pushes on the brain itself [1]. When drinking coffee this is the reason why there is vasoconstriction occurring.
cyclic Amp specific 3’5’ cyclic phosphodiesterase
How it works naturally:
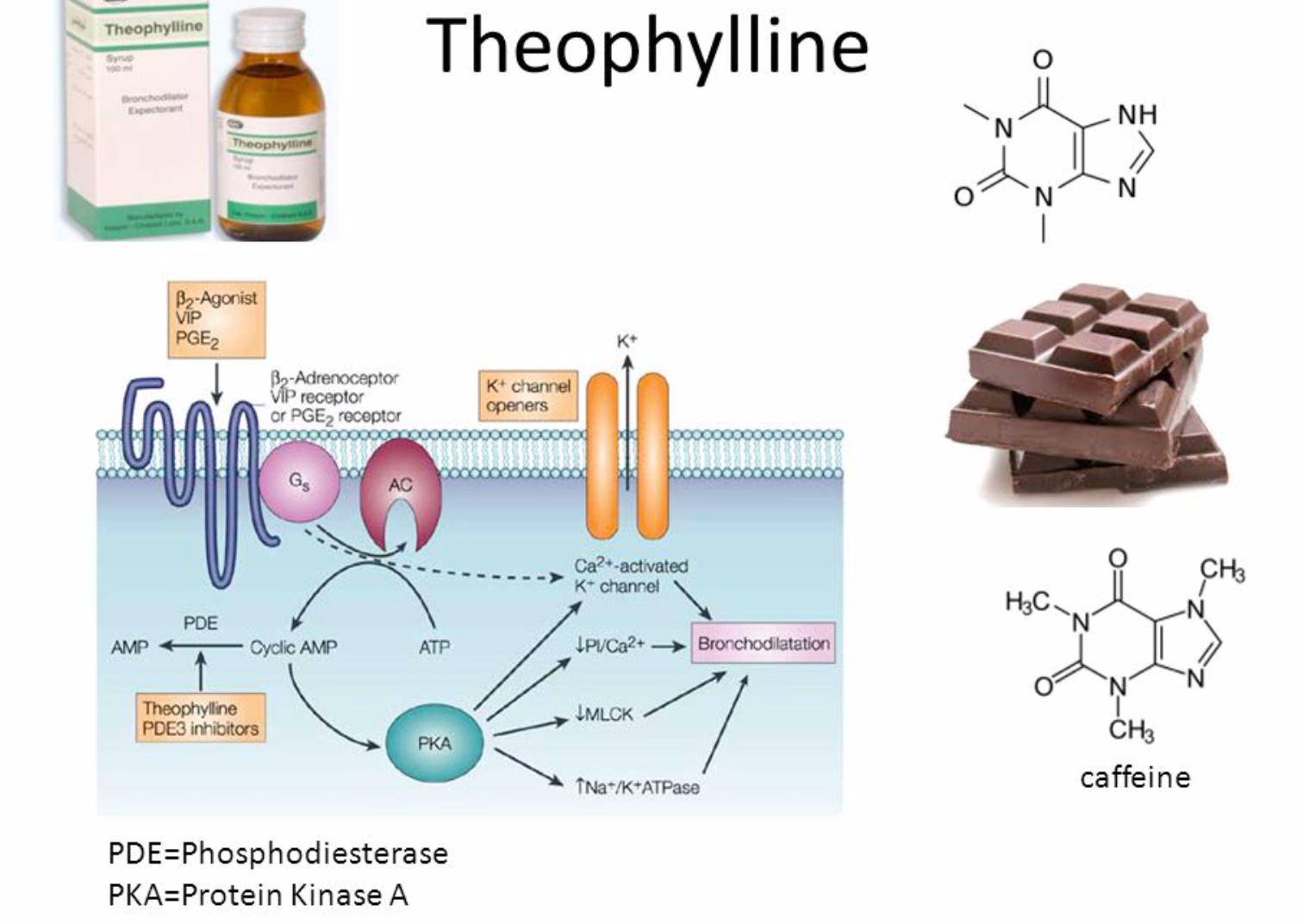
Figure 5. Demonstrate the pathway involving cAMP and second messengers.
This is different from the adenosine pathway. Normally the phosphodiesterase (PDEs) enzyme helps in regulating the amount of cyclic AMP (cAMP), which depending on their concentration, it will have different physiological effects. The PDEs degrades the phosphodiester bond of the cAMP and cGMP which are second messengers [9]. Essentially, second messengers regulate the localization, duration and amplitude of signalling within a cell [9]. It is very important to regulate these second messengers as they have a huge influence on the cell, hence PDEs play a huge role in regulation. In figure 5, you can see the cyclic AMP acting on the protein kinase A (PKA) which ultimately results in bronchodilation (this figure is just an example from theophylline that acts like caffeine).
How caffeine intervenes:
The caffeine molecule will block and inhibit the phosphodiesterase enzyme (PDEs) and an increase of the second messenger cAMP will occur. As the cAMP increases in concentration in the cell, it will create a prolonged and amplified response throughout the cell. Many pathways will be activated as the protein kinase will be activated which has an influence on many other pathways in the cell (sorry for not being specific but they are a lot of pathways, all connected and balanced with each other). For example, theophylline that belongs like caffeine in a xanthine group will inhibit PDEs enzyme and hence increase cAMP concentration. Using theophylline medically helps in chronic obstructive pulmonary disease, asthma and infant apnoea [10] and has the following effect:
relaxing bronchial smooth muscle,
increasing heart muscle contractility and efficiency,
increasing heart rate,
increasing blood pressure,
increasing renal blood flow [10].
Other receptors that caffeine acts on
Calcium Mobilization,
Benzodiazepine Receptors [1].
Conclusion
Widely loved in the world and taken daily by many people, we all enjoy what caffeine does to our body (or maybe some may not view it that way). We can say that caffeine acts quickly, rapidly absorbed, distributed well throughout the body and readily crosses cell membranes — although the experience may differ from individuals. It primarily inhibits our important phosphodiesterase enzymes and competes with our beloved adenosine molecule.
I hope that this blog has shed some light into the mysteries of caffeine and I will excuse myself as cappuccino is waiting for me to be absorbed, distributed, metabolised and excreted.
Published 15th February 2019. Last reviewed 30th December 2021.

Reference
1. Ncbi.nlm.nih.gov, 2001. Caffeine for the Sustainment of Mental Task Performance: Formulations for Military Operations. [Online] Available at: https://www.ncbi.nlm.nih.gov/books/NBK223808/.
2. Dr. Pete Johnson, 2018. Introduction to Pharmacology. Lecture given at James Cook University. Tuesday, 24 April 2018.
3. DrugBank, 2019. Caffeine. [Online] Available at: https://www.drugbank.ca/drugs/DB00201.
4. PubChem, 2019. Caffeine. [Online] Available at: https://pubchem.ncbi.nlm.nih.gov/compound/2519#section=Top.
5. Alcohol and Drug Foundation. Caffeine. https://adf.org.au/drug-facts/caffeine/. Accessed February 9, 2019.
6. Daly JW, Shi D, Nikodyivic O, Jacobson KA. 1999. The role of adenosine receptors in the central action of caffeine. In: Gupta BS, editor; , Gupta U, editor. , eds. Caffeine and Behavior: Current Views and Research Trends. Boca Raton, FL: CRC Press. Pp.1–16.
7. Daly JW. 1993. Mechanism of action of caffeine. In: Garattini S, editor. , ed. Caffeine, Coffee, and Health. New York: Raven Press. Pp.97–150.
8. Cardiovascular Pharmacology Concept. Adenosine. https://www.cvpharmacology.com/antiarrhy/adenosine. Accessed February 10, 2019.
9. Wikipedia. Phosphodiesterase. https://en.wikipedia.org/wiki/Phosphodiesterase. Accessed February 10, 2019.
10. Wikipedia. Theophylline. https://en.wikipedia.org/wiki/Theophylline#Medical_uses. Accessed February 11, 2019.
Figure 1. Drugbank Authors. Caffeine. Drugbank website. https://www.drugbank.ca/drugs/DB00201. Updated on January 23, 2020. Accessed February 10, 2019.
Figure 2. Ncbi.nlm.nih.gov, 2001. Caffeine for the Sustainment of Mental Task Performance: Formulations for Military Operations. [Online] Available at: https://www.ncbi.nlm.nih.gov/books/NBK223808/.
Figure 3. Wikipedia. Adenosine. https://en.wikipedia.org/wiki/Adenosine. Accessed February 10, 2019.
Figure 4. Richard E. Klabunde, Cardiovascular Pharmacology Concept. Adenosine. https://www.cvpharmacology.com/antiarrhy/adenosine. Accessed February 10, 2019.
Figure 5. Wikipedia Authors. Phosphodiesterase. Wikipedia website. https://en.wikipedia.org/wiki/Phosphodiesterase. Accessed February 10, 2019.
Table 1. Drugbank Authors. Caffeine. Drugbank website. https://www.drugbank.ca/drugs/DB00201. Updated on January 23, 2020. Accessed February 10, 2019.
Useful websites and links:
South African Medicine Formulary (SAMF),